
Muhammad Rafay and Areeba Tariq*,
Liaquat National Hospital.
Received Date: March 14, 2024
Accepted Date: May 09, 2024
Published Date: May 24, 2024
Citation: Muhammad Rafay and Areeba Tariq. (2024) “Solitary Cervical Spine Osteochondroma- A Rare Case Presentation.”, International Journal of Medical Case Reports and Medical Research, 2(4); DOI: 10.61148/2994-6905/IJMCRMR/034.
Copyright: © 2024. Areeba Tariq. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Osteochondroma was first described by Reid in 1843 [1]. It is a common benign bone tumor that contributes up to 15% of all bone tumors [2]. Frequent sites of involvement are the axial skeleton and metaphysis of long bones including the distal femur and proximal tibia [3-5]. Around 3 % of osteochondromas involve the spine [6-8]. Osteochondromatosis is used in case they are multiple [9].
Introduction:
Osteochondroma was first described by Reid in 1843 [1]. It is a common benign bone tumor that contributes up to 15% of all bone tumors [2]. Frequent sites of involvement are the axial skeleton and metaphysis of long bones including the distal femur and proximal tibia [3-5]. Around 3 % of osteochondromas involve the spine [6-8]. Osteochondromatosis is used in case they are multiple [9].
Around 7% of tumors are hereditary and involve the spine [10]. These tumors rarely cause spinal cord compression [2]. The involvement of osteochondroma in the cervical spine is unusual. It usually involves C1 and C2 but rarely involves subaxial cervical spine [11]. These tumors may cause a variety of symptoms ranging from root compression to vertebral fractures [12].
Case Presentation:
A 14-year-old male with no other known comorbid was admitted through OPD with a 10-year history of a mass lesion in the region of the cervical spine. Mass was initially smaller but attained a gradual increase in size with time. It wasn’t associated with any kind of pain or tenderness, nor did it show any kind of surrounding skin discoloration or temperature changes on examination. It was hard and irregularly shaped but there wasn’t any associated motor or sensory deficit.
MRI C-spine showed a mass lesion involving posterior elements of the C5-C7 vertebra. (Fig 1)
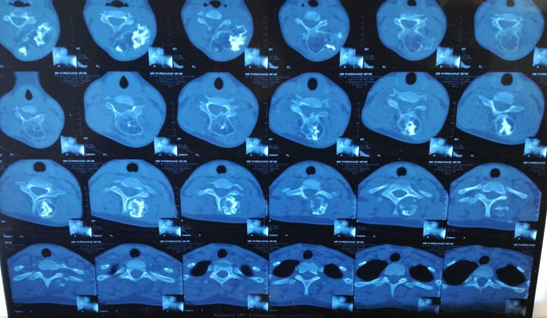
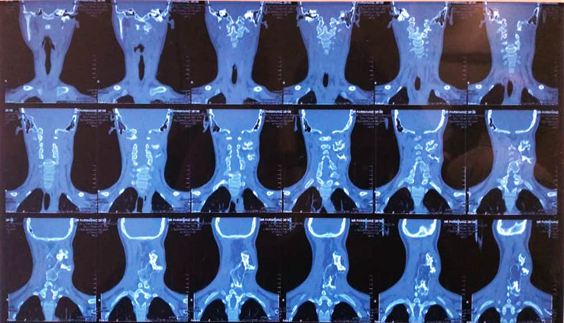
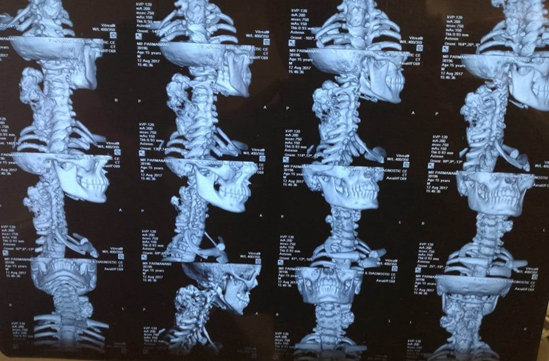
CT C-spine showed a bony mass of approximated measurement of 5 X 5 X 8 cm, arising from C6 lamina and involving C5 lamina.
The patient underwent C5-C6 laminectomy along with excision of C5-C6 facets, followed by total tumor resection. His intra-operative findings showed the mass to be encapsulated, lobulated, and yellowish in color while hard in consistency. It was mildly vascular expanding out between C2-T1 levels while showing attachments to C5-C6 lamina.
Histopathological studies showed the mass to be osteochondroma, a bony tissue with an outer fibrous perichondrium layer in continuation with the periosteum and an underlying hyaline cartilage cap revealing irregular calcification, myxoid degeneration, and few cystic spaces. (Fig 3)
The patient’s overall hospital stay remained uneventful, showing no signs of any neurological deficit.
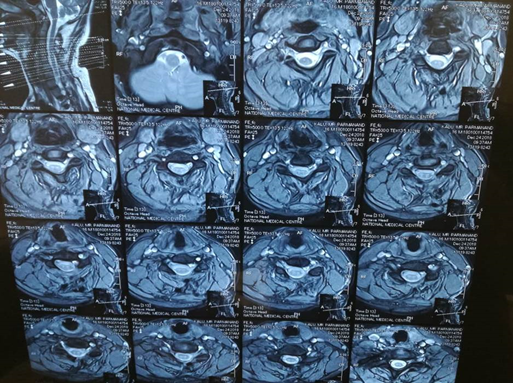
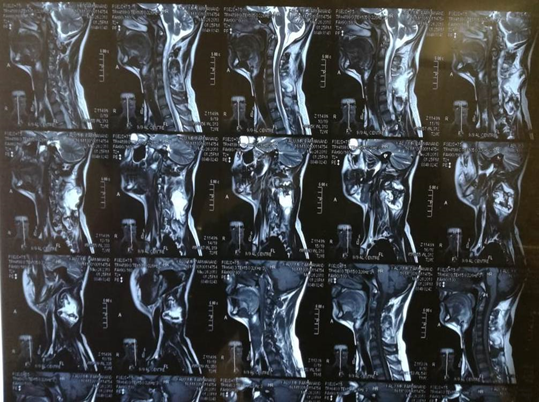
Figure 1: T2 weighted images of MRI cervical spine, sagittal and axial cuts.

(a)
(b)
(c)
 (d)
(d)
Figure 2: CT scan of the patient sagittal cuts (a), axial cuts (b), coronal cuts (c), and 3D reconstruction (d).
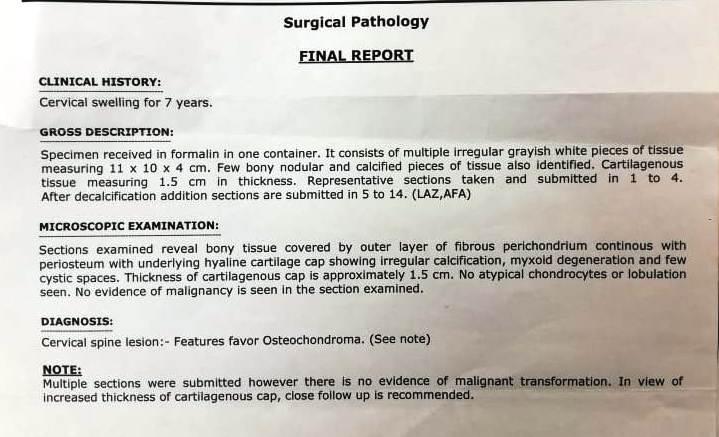
Figure 3: HISTOPATHOLOGY REPORT
Discussion:
As described earlier osteochondroma is an uncommon tumor of the cervical spine. It usually involves posterior spinal elements including the transverse process and the lamina of the spine [13]. According to the WHO definition, it is a benign cartilage-capped neoplasm of the outer surface of the bone [14]. It has an unclear pathophysiology, but ionizing radiation could be responsible for their growth [15]. Some studies also suggest the presence of an underlying trauma or congenital perichondral deficiency as a triggering factor [16].
The tumor has male preponderance and occurs in the second and third decade of life [17]. The development of exostosis is linked with cervical spine mobility. The most common vertebra involved in the cervical spine is C2 followed by C3 and C6 [18]. Cord compression is uncommon as these are exophytic lesions and tend to grow outside the spinal canal [19]. It causes a variety of symptoms including radiculopathy, myelopathy, or fracture of the vertebra. Plain radiograph is inadequate for the diagnosis [20]. CT scan is the imaging of choice, as it shows the full extent of the tumor and its relation to its surrounding structures. [21]. MRI on the other hand helps in analyzing neural structure involvement. Tumor appears hypo-intense on T1 weighted images and hyper-intense on T2 weighted images [22].
Asymptomatic lesions can be followed with time and surgery should be considered for intractable pain, for the neurological deficit, or for confirming diagnosis [23]. Radicle excision must be considered as incomplete excision leads to recurrence in up to 5% of the cases [17] To prevent recurrence one must completely remove the cartilaginous cap [24].
Conclusion:
Solitary spinal osteochondromas are an uncommon entity. They are considered benign neoplasms of the bone and rarely cause any neurological deficit because of their exophytic growth. Treatment is complete excision incomplete removal is liable for recurrence.

Open Access By Aditum Open Access Journals id licensed under Creative Commons Attribution 4.0 International License. Based On a Work at aditum.org